Annotation 4 & Experience
1) Objective: Understand and Evaluate an early intervention client (ages 0-3) who receives speech and language therapy services using the Mullen Scales of Early Learning Assessment.
Activities and Resources
- Research will be carried out through direct observation of the evaluation being performed on multiple clients and through direction and assistance from the internship supervisor.
- Use examiners manual as a guide on how evaluation should be administered, in what atmosphere, and how to record results.
- Resources include (but are not limited to):
- My supervisor, Joy Munson
- The Mullen Scales of Early Learning Assessment and Assessment Guide/Manual
- The accompanying kit of materials needed to administer the evaluation
- Online resources, such as the Mullen Assessment website.
Evidence:
- Gather all information I used for learning the assessment to include in my portfolio.
- An overview of the assessment, accompanying kit, and materials as well as how it will be performed/was performed.
- A completed Mullen assessment of an anonymous early intervention client
Evidence
Assessments and evaluations are the basis of all treatment and lesson plans, regardless of the discipline being addressed. After my past internship in the school system and seeing the evaluations performed at the elementary level, I was already aware that evaluations were a necessary part of speech therapy. I was able to expand my knowledge of evaluations through my second internship at Children's Friend. Early intervention is for children ages birth to three years old. Thus, the assessments used to evaluate the clients are those geared towards these ages. The assessment that I found to be the most pertinent and beneficial within the world of Early Intervention was the Mullen Scales of Early Learning Assessment.
I was able to observe my supervisor perform the Mullen Assessment on numerous occasions. The assessment is performed on all clients where a speech and language consult/referral is requested. The Mullen evaluation is a "global" assessment and looks at the child as a whole. It covers 5 basic areas of development: gross motor, fine motor, visual reception, receptive language, and expressive language. Even though for a speech consult/referral, the main area to be observed is the expressive and receptive language, and overall view of the child can all the SLP and other team members to identify a developmental issue that would be affecting multiple areas. One of the most difficult obstacles that I encountered while performing the Mullen was that many children get "stage fright" so to speak and are unwilling or too shy to perform the tasks requested of them. Many parents, when seeing that their child isn't performing the tasks at hand are eager to tell the SLPs and team members that the child is capable of performing said task. Unfortunately, scores are recorded for what the child is able and willing to do at the time of the evaluation, not what they are able to do when the assessment is not being performed. This however, can work to the advantage of a child who has border-line scores for qualifying for early intervention services. For example, if a child has scores on the Mullen below the average mark (at least 2 scores in different areas below average), they qualify for early intervention services. Some children with border line scores "fall between the cracks " so to speak and do not receive the assistive services that they are actually in need of.
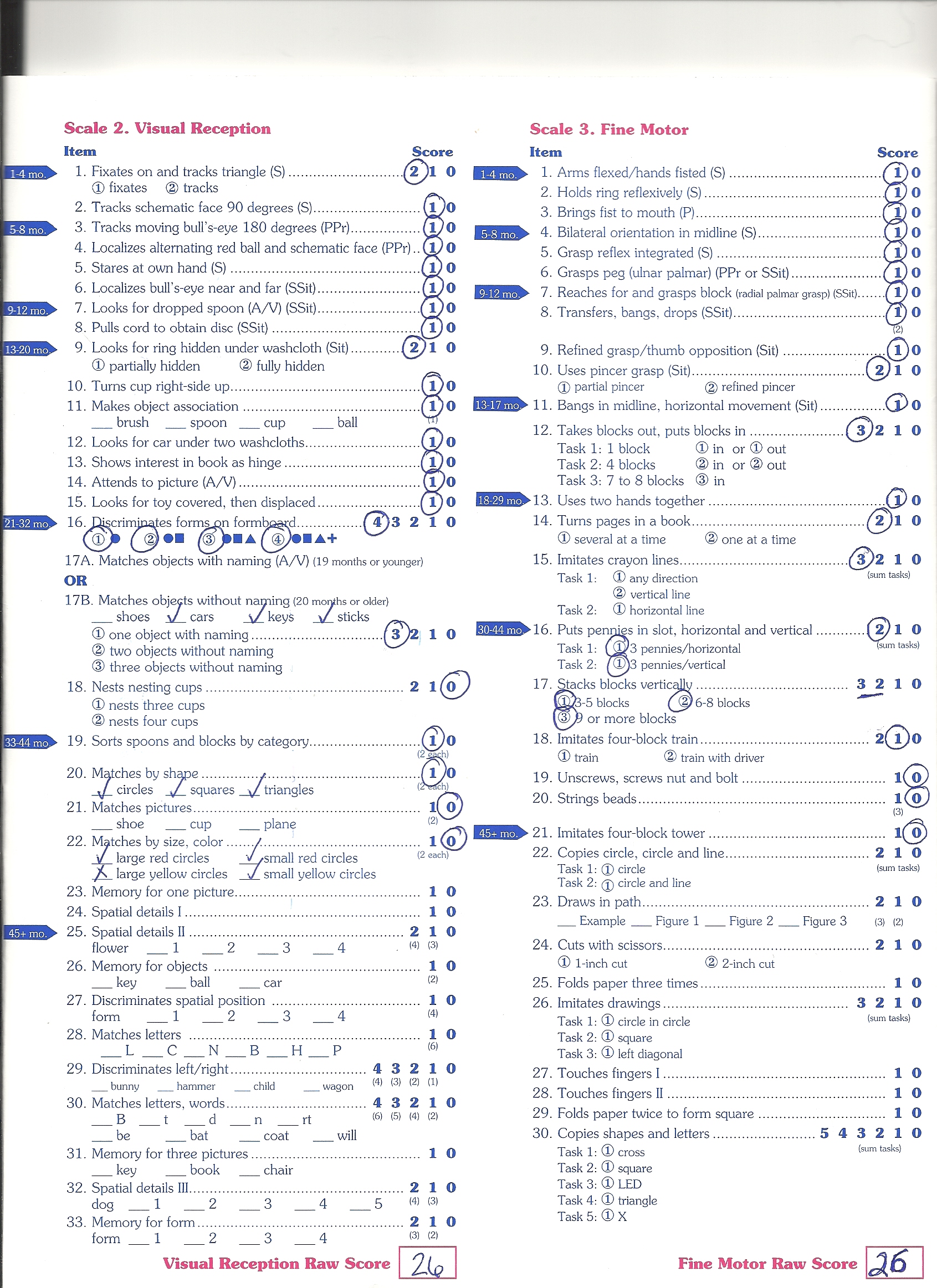
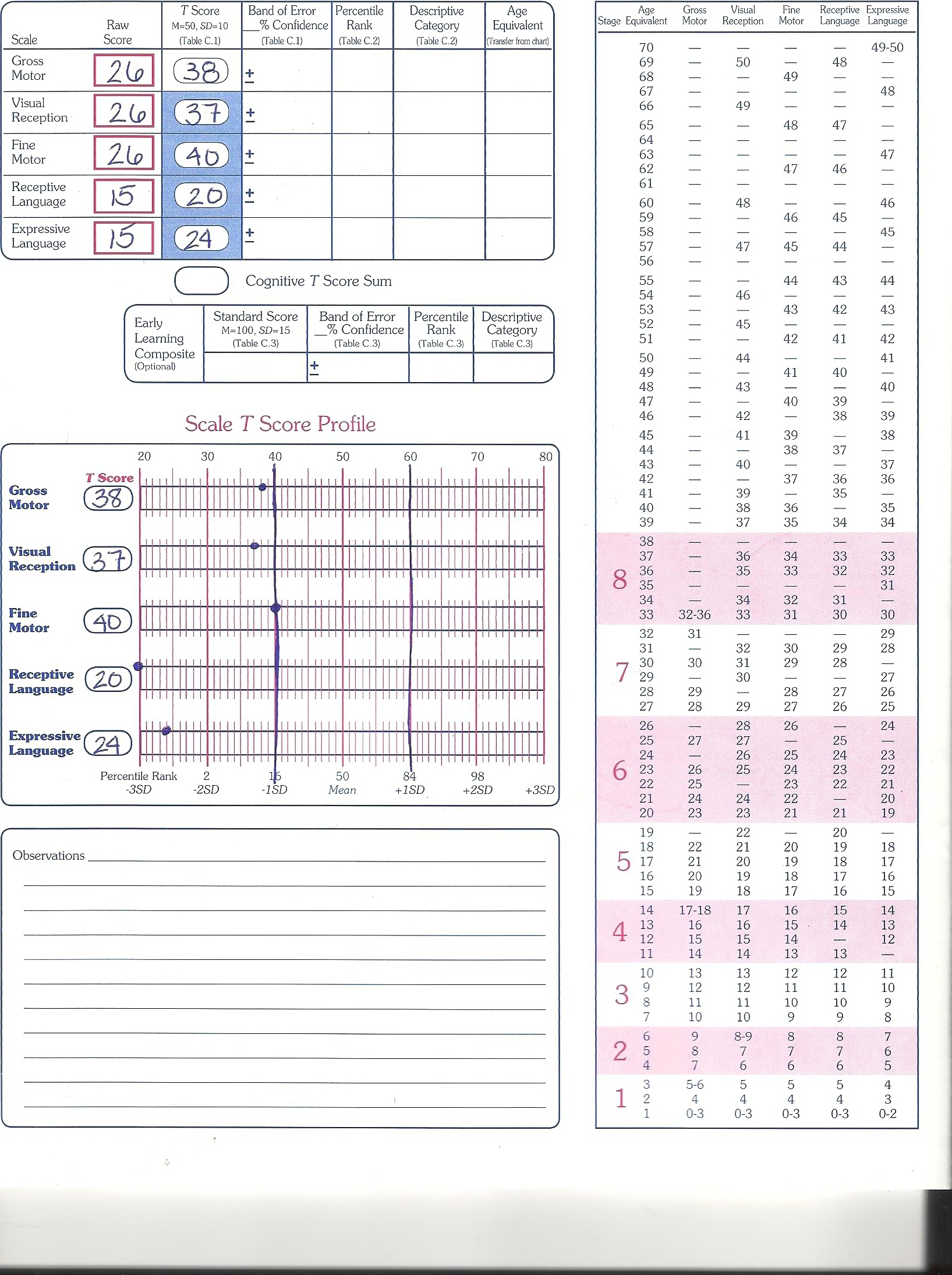
The child whom I assisted in the Mullen Assessment for was a 2 and a half year old boy with significant delays in all areas covered, except for the Fine Motor section in which he scored on the low-end of the Average area. The way the Mullen is conducted and scored is based up "Basal" and "Ceiling" Levels. The examiner (in this case the SLP and myself) needs to establish a basal level and a ceiling level. The Mullen will define both the levels in terms of correct and incorrect scores. A basal score is the entry level and the ceiling score is the test-terminating score ( i.e the point at which th of the child is unable to carry out any more of the tasks correctly). In many relatively long tests, like the Mullen, testing may begin at some arbitrary level judged appropriate for the child, instead of at the very beginning of the test. This will help save test administration time. If the judged entry level proves wrong, the clinician may move down to find the basal level. In the Mullen Assessment, a basal score is defined as 3 consecutive items with at least 1-point scores. If at the initial level of testing, a child scored only 1 out of 3 responses correctly, the judged entry level would have been too high; the examiner then moves down the test items to find the first 3 consecutive items with a score of 1 point. Once a basal is established, all test items prior to it are considered correct and the testing continues forward. A ceiling in the Mullen is defined as 3 consecutive items with scores of 0. The ceiling represents the highest number or level of test items administered or the point at which the test administration is stopped because the remaining higher level items are all considered failed. A test may require that a basal and ceiling be established to calculate a raw score.
The Mullen Scale is used for the assessment of the cognitive functioning of young children. The assessment is centered around the child’s responses to activities prepared by the examiner and outlined by the kit. The Mullen Scales measure five distinct skills which are: Gross Motor, Fine Motor, Visual Reception, Receptive Language, and Expressive Language. The "global" intellectual performance is measured with the Mullen and an overall picture of the child is created based on their response to activities. The gross motor scale is administered to children from birth to 33 months and the four “cognitive” scales are administered to children from birth to 68 months. Mullen scale scores can be used to identify children with special education needs who are eligible for further evaluation and in this case, eligibility for Early Intervention services. The normative scores can also provide an objective means to identify weaknesses and strengths that underlie a child’s learning style for the purpose of designing individualized instructional plans that capitalize on the child’s strengths. For early intervention, these scores are used to assist in the development of an Individual Family Service Plan (IFSP).
Scoring of the items on the scales is provided by the "Item Administration Book" (which is included in the kit when it is purchased.) Scoring is done on a record form containing a list of tasks and/or stimuli of possible responses for each assessment item. In most cases, the child receives a “1” for correct responses and “0” for incorrect responses. In some cases, the tester must sum the task scores to obtain the item scores. For each scale, the raw scores are then converted into age-adjusted normalized scores. The four “cognitive” skills T score can be further converted into a normalized ELC score. This ELC score has a mean of 50 and a standard deviation of 10. The scores can be used obtain the child’s percentile rank and age equivalent score, the age at which the child’s raw score is the median score.
Each scale is administered individually and is not timed. For some items on the scales, the questions are geared towards the parents and for some, a parent's assistance may be used to encourage a response from the child. Administration of the evaluations varies by age, anywhere from 15 minutes to 60 minutes. The materials used for the assessment are an examiner's manual, an administration book, a stimulus book, protocols, and the kit consisting of many toys.
The Gross Motor Scale consists of 35 items and is to be used only through 33 months of age. The child's skills examined are assessed in supine, prone, sitting, and upright positions. The skills range from rotating of the head to hopping on one foot.
The Visual Reception Scale is concerned primarily with discrimination and memory. The scale is comprised of 33 items which range from tracking to remembering various forms.
The Fine Motor Scale has 30 items which asses skills from evidence of specific reflexes to drawing a triangle.
The Receptive Language Scale consists of 33 items as well It looks to assess comprehension and memory of the child. The skills being examined range from a reflexive reaction to a loud noise up to identifying letters.
The Expressive Language Scale is made up of 28 items which tap into language production as a whole. The skills which are tested on this scale range from evidence of a sucking, swallowing, and chewing movements to repeating sentences up to 12 words long.

A multidisciplinary evaluation is conducted to determine the child’s initial eligibility for the Early Intervention Program. It is also used to identify the services required to address the child's specific developmental needs. In addition, the family’s information regarding the child including the resources, priorities, and concerns of the family and supports or services necessary to enhance the family’s capacity to meet the developmental needs of the child are determined. Family involvement to assist with the design of the comprehensive evaluation and intervention strategies is an integral part of the evaluation process. As stated earlier, Early Intervention is family-centered so the more involved the family is, the more beneficial the program will be for their child.
The multidisciplinary team from Children's Friend, which considers the multidisciplinary evaluation of the child and subsequent recommendations, family information, parent recommendations, observational information, and professional judgment determine whether the child meets the criteria for Early Intervention.
The evaluation of the child must be based on the following:
- A review of pertinent records related to the child’s current health status and medical history.
- An evaluation of the level of functioning, as needed; in cognitive development, physical development including vision and hearing, communication development, social/emotional development, and adaptive development.
- An assessment of the child’s unique needs in terms of developmental areas and identification of services appropriate to meet those needs.
- A summary of the family’s information regarding the child.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}